
Oral hygiene is an everyday routine. A toothbrush, a little toothpaste, a few quick movements, and at the end often a dose of "reassurance": a disinfectant rinse, fresh breath and a clean feeling. The modern hygiene approach is simple: whatever is antibacterial is useful. A microbiome-based view, however, places the situation in a different perspective: the mouth is not merely an opening but an actively functioning ecosystem, capable of causing inflammation and of steering biochemical processes.
The turning point comes when, alongside eliminating pathogens, we also consider the importance of preserving so-called beneficial functions. In the mouth there are not just two opposing groups; a community forms in layers and biofilms, with continuous metabolism. When we intervene in this system, it is not simply a matter of updating a list of microbe names. In reality we also bring about changes in the functioning of the host organism.
One of the finest examples is the so-called enterosalivary nitrate–nitrite–NO cycle. Nitrate from the diet — typically from green leafy vegetables and beetroot — enters the circulation. The salivary glands do not simply let it circulate: they concentrate it and secrete it into the saliva. So far this is only logistics. The decisive step takes place in the mouth.
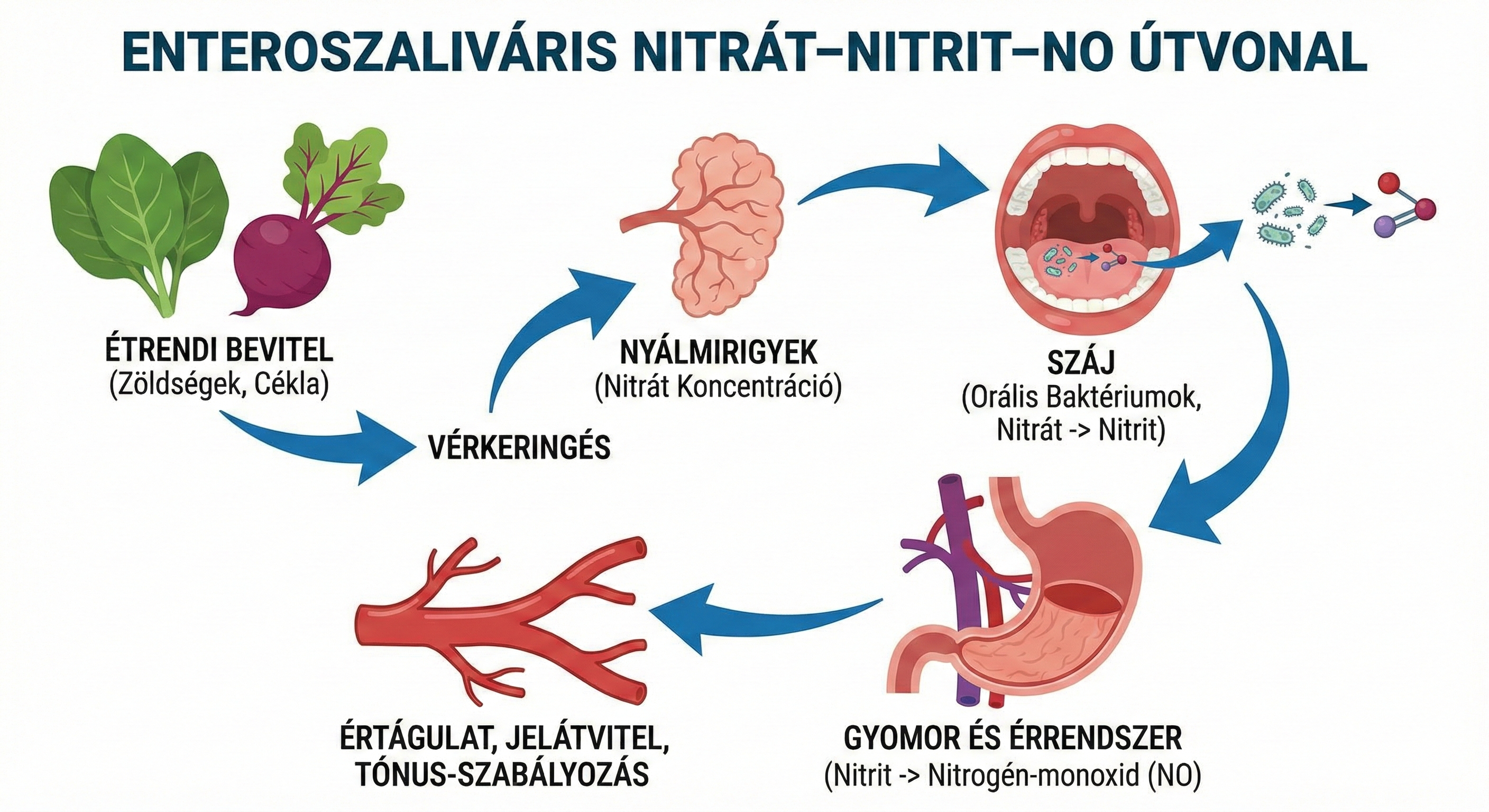
The nitrate-reducing communities of the oral cavity convert nitrate into nitrite. After being swallowed, nitrite contributes through several routes to the bioavailability of nitric oxide (NO). NO plays an important role, as it contributes to the dilation of blood vessels, the regulation of vascular tone and various signalling processes. This circulatory system is not the task of the liver alone, nor does the endothelium solve the problems by itself. One of the entry points in the cycle's processes is the mouth, whose "door handle" is microbial in nature.
Within this framework mouthwash is not a cosmetic but a potential signalling-pathway inhibitor. Strongly antibacterial, disinfectant rinses do not discriminate between the "unpleasant" and the "beneficial": they can also reduce the nitrate-reducing communities. As a consequence, the oral nitrogen cycle may narrow, which can result in decreased nitrite formation, and at the same time it can obstruct one of the important nutritional channels of the NO pathway.
The mechanism is best revealed in human research, where the rise in salivary and plasma nitrite levels is observed after nitrate intake. With antibacterial mouthwash use, nitrate still reaches the saliva, but nitrite formation can be significantly reduced or even abolished. This clearly indicates that the physiological activation of dietary nitrate largely takes place in the mouth.
The most frequently cited intervention results concern chlorhexidine (CHX). With short use over a few days or weeks, the amount of nitrite in the saliva can drop significantly, and the circulating nitrite level is also reduced. In a human study of 19 healthy volunteers, 7 days of chlorhexidine rinsing reduced oral nitrite production by roughly 90%, plasma nitrite fell by about 25%, and in parallel systolic/diastolic blood pressure rose on average by ~2–3.5 mmHg; the change in blood pressure went hand in hand with the drop in circulating nitrite. A small but measurable shift has also been described in treated hypertensive patients: in a 15-person, randomised, crossover study, 3 days of antibacterial mouthwash was associated with an average +2.3 mmHg systolic increase compared with the water control (95% CI 0.5–4.0), in parallel with the weakening of the nitrate→nitrite conversion. At the same time, several studies show that this may be accompanied by a small rise in blood pressure. Generally this means an increase of about a few mmHg. This does not represent a major clinical problem for most people, but it is not physiologically negligible, and if we consider the population as a whole, "small but sustained shifts" always matter.
The situation is not clear-cut. There are studies suggesting that although the biochemical signal — that is, the decrease in the conversion of nitrate to nitrite — can be tracked, blood pressure nevertheless shows no measurable change. This applies mainly to young and healthy groups, over a short period. At the same time, responses can differ significantly between individuals: while in some the same intervention may produce a positive change, in others no difference is detectable, and in certain cases even opposite effects may appear. This variability is not merely a random phenomenon but a fundamental feature of the microbiome. The baseline state is a significant factor: the biofilm layer on the tongue, tongue-cleaning habits, dietary nitrate intake and compensatory physiological processes all play a role in it. Moreover, disinfection does not affect only a single channel. During chlorhexidine use, shifts in the salivary microbiome as well as changes in pH and buffering capacity have been observed. Together these underline that a mouth rinse is not just a specific treatment but also an ecological intervention.
Many have tried to uncover the long-term effects through observational research. There are data showing that using mouthwash several times a day can be associated with a more frequent occurrence of hypertension in certain groups. This, however, is only an association: although certain confounders can be corrected for, the results do not provide causal evidence as strong as a comprehensive, long-term randomised trial. Consequently the final picture cannot be a clear-cut statement. Some pooled analyses do not detect a statistically significant, uniform rise in blood pressure with mouth-rinse use. At the same time, mechanistic reviews consistently indicate that nitrate/nitrite markers decrease with antibacterial rinsing, and this has been observed in several human experiments. The rise in blood pressure and the biomarker pathway can be observed simultaneously. The two can coexist. The biomarker pathway is real, whereas the clinical endpoints are not always valid, since they depend greatly on the agent used, the dose, the duration and the underlying condition.
The misleading part of the story lies in labelling mouthwash as generally bad, so that many may think the only solution is to abandon mouthwash entirely. Another aspect of oral hygiene is also extremely important: consensus reports indicate a strong epidemiological link between severe gum disease and systemic cardiovascular risk. Furthermore, numerous meta-analyses have shown that periodontal treatment produces a moderate improvement in inflammatory markers and in systolic blood pressure as well. In periodontitis, several diseases can co-occur. Oral inflammation can be a chronic low-grade source of inflammation, the treatment of which is not merely an aesthetic question but is also highly important for preserving systemic health.
For precisely this reason, the correct priority does not begin with the use of mouthwash. Reducing inflammation in the oral cavity is achieved primarily through the mechanical removal of plaque and through dental and periodontal care. Mouthwash can at most be a supplementary, targeted tool, but it does not replace the basic hygiene practices.
We are happy to answer your professional questions — we respond to every enquiry.
Write to us