
Studies of recent years make it increasingly clear that reaching an optimal vitamin B12 level in the body depends not only on adequate intake but also on the vitamin's efficient absorption. As medicine has advanced and the standard of healthcare has risen, life expectancy has increased significantly — and with it the importance of the chronic conditions that impair quality of life in old age. Over the past decades we have recognised the important role of vitamin B12 in the ageing process. At the same time, assessing B12 status poses a serious problem, because a true gold-standard laboratory measurement is lacking. The clinical manifestations of severe B12 deficiency have long been known (pernicious anaemia, irreversible neuropathy), but we are also gaining ever more knowledge about the changes caused by subclinical deficiency.
Vitamin B12 can exist in several chemical forms; it has two known activated forms: methylcobalamin and adenosylcobalamin. Its synthetic version is cyanocobalamin, and this is usually the compound contained in the medicines, vitamin preparations and dietary supplements intended for B12 replacement.
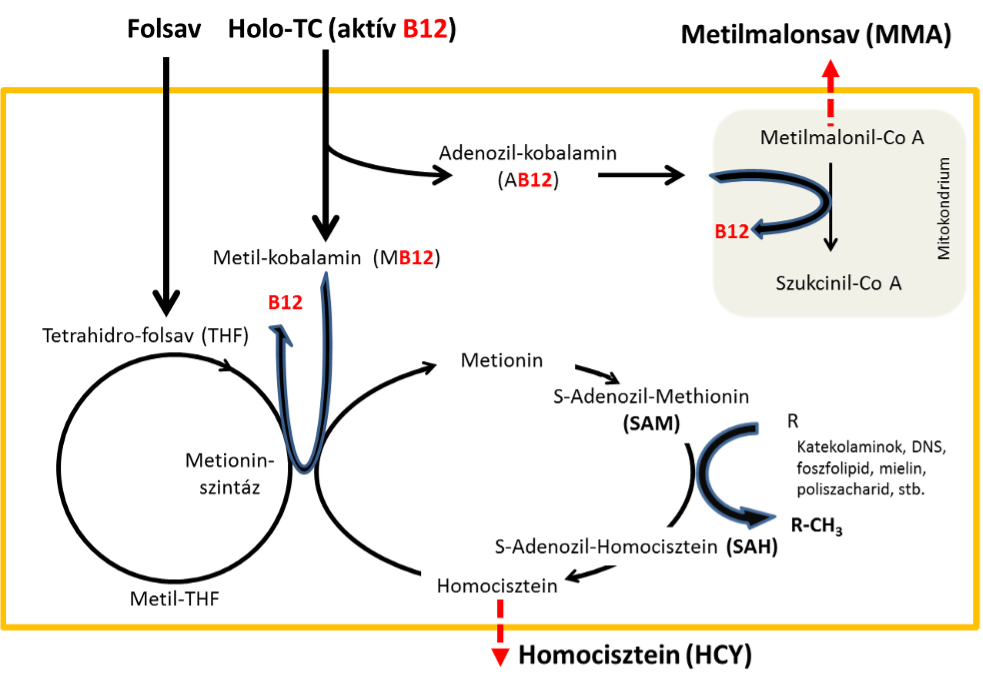
B12 acts as a coenzyme for two important enzymes: methionine synthase and methylmalonyl-CoA mutase (1). These enzymes play a central role in the metabolism of branched-chain amino acids and of long-chain fatty acids with an odd number of carbon atoms. In the absence of the B12 coenzyme, the reduced activity of the two enzymes leads to a rise in methylmalonic acid (MMA) and homocysteine (HCY) levels, and these substances also show elevated values in the circulating blood (2). As a consequence of the rise in MMA and HCY, total cholesterol also increases. A very important consequence of B12 coenzyme deficiency is the disturbance of intracellular methylation processes: this affects phospholipid methylation as well as the methylation of neurotransmitters, biogenic amines, DNA and RNA, and myelin basic proteins. (Figure 1: The main intracellular roles of vitamin B12 and folate).
The fundamental biochemical processes taking place in cells can also be greatly influenced by the combined status of vitamin B12 and folate. In B12 deficiency, even if sufficient folate is available, the inactivity of methionine synthase reduces the amount of usable tetrahydrofolate (THF), while the available folate is converted into the inactive methyl-THF form. As a result, cells suffer from folate deficiency despite an adequate supply of folate (3). DNA synthesis halts, which first causes symptoms in the most rapidly dividing cells: erythropoiesis in the bone marrow undergoes megaloblastic transformation, megaloblastic haematopoiesis may develop, and ultimately pernicious anaemia. In this case the serum folate laboratory test may show an adequate concentration, yet the folate level of the red blood cells can be low. With B12 replacement the methionine synthase enzyme is activated and folate metabolism normalises — the relative folate deficiency can resolve even without folate administration.
The absorption of vitamin B12 is a highly complex process and depends greatly on the functioning of the digestive system. As age advances, the efficiency of B12 absorption declines. It is contained in food of animal origin (which is why B12 deficiency is considerably more common in vegetarians (4)), and the B12 occurring in food is strongly protein-bound, so healthy gastric and peptic digestive processes are required to release it. Synthetic B12 taken orally is present in free form, so its absorption does not require vigorous gastric digestion. Free B12 binds to the R-protein originating from the stomach, and then in the duodenum Intrinsic Factor (IF) attaches to it. The B12–IF complex is absorbed in the terminal ileum through an active, calcium-dependent process. Absorption is accordingly regulated in several ways — the amount of IF and the quantity of the calcium-dependent receptor molecules are the most important regulators.
Absorbed B12 can bind to two transport proteins: the larger part of B12 (70–80%) binds to a protein called haptocorrin — which, according to current knowledge, is inactive and does not participate in cellular metabolism; the smaller amount of free B12 binds to the protein transcobalamin, forming the biologically active holo-transcobalamin (HTC) molecule. B12 molecules are mostly stored in the liver, and they reach the body's cells in the HTC form, carried by the circulation. The body's B12 metabolism is characterised by great inertia: its deficiency may take years or even decades to develop, but eliminating the deficiency also requires a longer time. Numerous studies have shown that, in the long term, high-dose oral B12 replacement is more effective and more successful than parenteral B12 administration.
Over the past decades several methods have been available for the quantitative determination of all the B12 molecules present in serum. The protein-binding-based chemical quantification of B12 has become a stable, everyday routine; however, the result obtained very often did not correlate with the clinical picture or with the B12 value expected on other grounds, for example on the basis of red blood cell morphology. As a consequence, the value defined as the decision threshold for B12 deficiency may vary from laboratory to laboratory — in the literature it ranges between 100 and 300 pmol/L. On this basis it is clear that the total B12 level measured in serum does not consistently reflect the actual intracellular B12 status.
In the absence of vitamin B12, the methylation conversion of homocysteine to methionine is disrupted, so one sign of intracellular B12 deficiency is the rise in plasma total HCY and MMA levels, and as a consequence of their elevation total cholesterol also rises. On its own, however, HCY determination is still not suitable for assessing the cells' B12 status — alongside high sensitivity it has very low specificity, since a deficiency of other substances can also cause an increase in HCY. HCY elevation is caused by folate deficiency, vitamin B6 deficiency and riboflavin deficiency. It is also affected by the sex, age and renal function of the person examined, and genetic factors can influence it greatly as well. It is important to know that after blood sampling, HCY determination requires increased attention, because in the blood drawn into the tube large amounts of HCY may be released from the red blood cells while it stands. Using a gel blood-collection tube and rapid separation after sampling, the pre-analytical accumulation of HCY can be prevented. According to the practice of recent years, however, HCY measured in a carefully collected sample is an early and highly sensitive marker of intracellular B12 deficiency (5).
MMA determination has not become widespread in practice. Methods exist with which plasma MMA levels can be measured well, and daily MMA secretion can also be determined in collected urine. The drawback of MMA determination is that its specificity is equally low — that is, not only a decrease in intracellular B12 can cause an MMA rise. However, the reverse of the statement is true: a decrease in intracellular B12 is always accompanied by a rise in MMA.
Since the total B12 level measurable in serum, as well as the HCY and MMA determinations used as functional tests, were not sufficiently specific, an analytical method was developed for the quantitative determination of active B12, the holo-transcobalamin molecule. With this method, which determines the HTC level in blood serum drawn during a simple blood test, the body's B12 metabolism can be followed effectively and accurately, and the cells' B12 content can be assessed. Numerous studies have shown that a low HTC level is clearly associated with a B12-deficient state of the cells. Low HTC levels have been found in vegetarians, the elderly, in cases of B12 malabsorption, in age-related cognitive decline, and in presenile dementias (e.g. Alzheimer's disease), etc. The HTC level can be slightly influenced by renal function and by certain hereditary factors. Overall, however, it can be stated that of the laboratory methods currently available, HTC determination most accurately indicates the state of intracellular B12 metabolism.
The relationship between vitamin B12 deficiency and elevated HCY is prompting more and more researchers to study the connection. Where the HCY rise has a hereditary genetic cause, the affected patients more frequently develop cardiovascular disease. According to several studies, a reduction in HCY produced a statistically significant decrease in the development of heart disease and stroke. According to recently launched and still ongoing studies, substantial oral intake of vitamin B12 greatly reduced the risk of stroke in patients who had low active B12 and high HCY levels at the start of the study (6).
According to some studies, the combined use of B12 and folate improved circulation in the coronary arteries of the heart. These results are promising, but many further studies are needed to settle the question conclusively.
The relationship between mental performance and vitamin B12 status has likewise been the subject of study for many years. Elevated HCY has for years been among the diagnostic criteria of Alzheimer's disease. Numerous studies have shown that in people found to have a lower HTC (active B12) level and an elevated HCY level in their forties and fifties, the chance of developing dementia — and thus Alzheimer's disease — increased significantly. If the HCY level can be reduced by 3 µmol/L (for example with oral B12), the risk of developing dementia can be lowered by 22% (7). Numerous randomised clinical trials are under way regarding the effect of B12, folate and other members of the B-vitamin group on early cognitive decline, focusing on cognitive performance (8). It is also an important finding that late-life depressive states respond very well to oral vitamin B12 replacement (9).
A lower level of bone metabolism causes decreasing mineral density in the bone tissue and can ultimately lead to osteoporosis. Low serum HTC and elevated HCY show an association with lower bone mineral density. When B12 is low the risk of bone fracture rises — and all this can be prevented by B12 replacement. The relationships between bone metabolism and vitamin B12 are likewise the subject of prospective clinical studies currently under way (10).
In summary, it can be stated that extensive investigation of the cellular biochemical processes of vitamin B12 and folate has revealed many new connections. In the near future, vitamin B12, folate and further members of the B-vitamin group may well have a new role in the prevention of cardiovascular disease, in maintaining mental performance, in preventing dementias, and in maintaining optimal bone density.
We are happy to answer your professional questions — we respond to every enquiry.
Write to us